
Two Million Screenings In: UE LifeSciences Wants Painless Detection to Be the Norm
By Arunima Rajan

In an interview with Arunima Rajan, Gauri Navalkar-Godse, CEO of UE LifeSciences, says the iBreastExam is the first line of defence when it comes to detection
Where are you from, and what drew you to this profession?
My grandmother was a doctor, so I was drawn to the profession thanks to her. I spent over a decade studying and working in the US. One of the key things I realised, living in the US versus India, is that the focus on preventive healthcare is very low here. When you see how that affects people's overall health, late diagnosis versus early diagnosis, you realise why a healthcare system that prioritises early detection is irreplaceable. India being home ground, I wanted to bring back a technology that would create a widespread impact. UE LifeSciences fills exactly that gap.
What is UE LifeSciences, and could you explain how your flagship product, iBreastExam, works? What specific problem are you trying to solve?
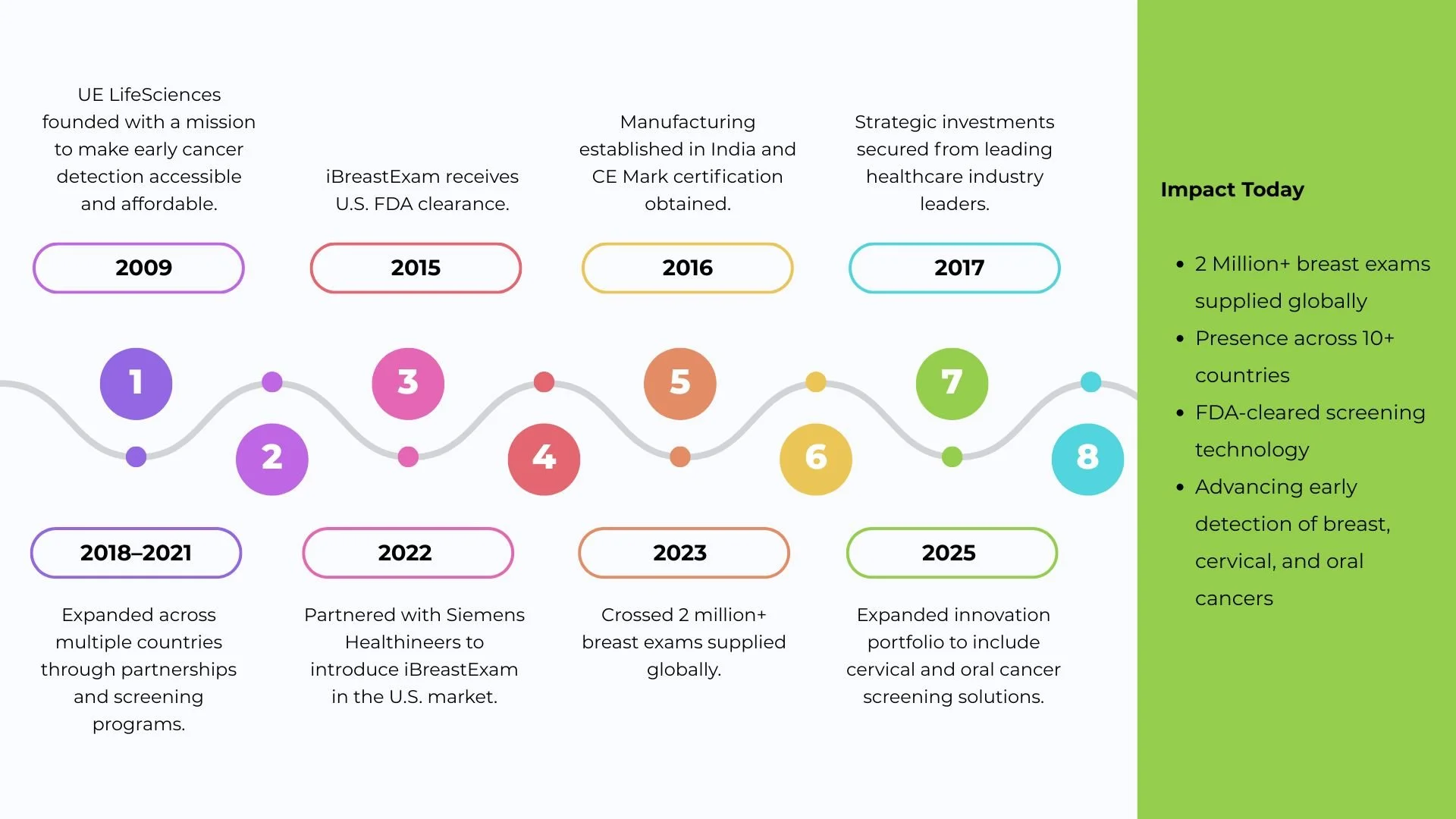
UE LifeSciences is a health company making the early detection of cancer accessible. It is focused on Femtech, primarily through our flagship product, the iBreastExam, which is a hand-held device. When we looked at breast cancer in India, we realised there were many challenges. First, there is a shortage of radiologists needed to read mammography results. Second, mammography uses radiation, which limits its usage to women above the age of 45, yet we see the occurrence of breast cancer in far younger women as well. Third, younger women tend to have a higher percentage of dense breast tissue, which often renders mammography results inconclusive in these cases.
We aren’t replacing mammography, but from an early detection perspective, you need a technology that can be applied across multiple age groups and demographics. That’s the gap the iBreastExam is looking to bridge.

Can you explain the core differences between Mammography and the iBreastExam?
Mammography is more comprehensive and requires infrastructure. You need a highly skilled technician, and you need a radiologist to read the report. Plus, mammography uses radiation, which limits the age group that can get tested. For women in their 20s to 40s, mammography is not recommended as a preventive checkup.
In the case of breast cancer, there are really no symptoms in the early stages. However, it has the highest survival rate—almost 90 per cent—when detected in early stage one, making it highly treatable if caught early. We needed a technology able to address this, and that’s the FDA-approved iBreastExam.
You mentioned that the iBreastExam is less painful than mammography. Can you elaborate on that?
Absolutely, it's less painful because it takes only about 10 minutes and doesn’t involve the discomfort of mammograms. It literally feels like a stethoscope being placed on your breast. There is no pain or pressure applied, so it's quite user-friendly.
We've been talking to a lot of older women who have had a mammography, and the process really bothers them: having your breasts pressed between two cold metal plates and experiencing pain while being screened makes the procedure quite intimidating. In fact, most of the women I know have refused to take a mammography recently, despite having one two years ago, simply because they couldn't come to terms with the experience.
According to a longitudinal aging study conducted in India to observe mammography uptake, the results are shocking: it is only in the range of 1.3 to 1.7 per cent. We are talking about the 45 to 59 age group, who are most likely to develop breast cancer. Women younger than this are equally exposed, yet they have no ready opportunity to be screened at all. Mammography works amazingly well as a secondary screening device. If we screen with the iBreastExam device and an area is identified with positive findings, a mammography serves as a great further diagnostic tool to look into the BI-RADS category and confirm the follow-up clinical process.
Having been with the company for over 10 years, what keeps you motivated and excited?
It's the journey we have made, the women we meet, and every group we convince of the importance of early detection. A close friend of mine stopped taking mammographies five years ago because it was too painful and made her anxious throughout the process. Instead, she used to get the iBreastExam checkup done on a year-on-year basis. Last year, we detected the cancer. She followed this up with a mammography and an ultrasound, which confirmed it was a stage-I malignancy. Following this, she had surgery, chemotherapy, and the whole treatment.
Thankfully, because it was an early-stage detection, she didn't experience the regular side effects of losing massive amounts of hair or skin discoloration. When you see such cases—these women fighting breast cancer and coming out stronger—it sends a strong message that breast cancer does not mean the end of life.
While you have completed 2 million screenings, millions of women remain unscreened. How do you plan to scale up this coverage?
We've been working with a lot of partners, and the idea behind that is: why wait for a woman to come to a hospital if you can take the device to them? It takes about 7 to 10 minutes to get them screened in the medical facility of their office, and if there's a requirement for a follow-up, they can be referred to nearby hospitals for whatever clinical workflow needs to be followed.
The most important thing for us is that the women who got screened have come back and reached out again and again to get a checkup done every year. This number has been growing as they recommend the test to a friend, their mothers, or their sisters. This word-of-mouth marketing is very promising; it is women who are using it, feeling confident enough to talk about it to other women.
Could you elaborate on your operational model and how you utilize community networks?**
One of the biggest challenges we are facing in India is the number of radiologists. In the US, they have one radiologist per 10,000 people. In India, it's one radiologist for one lakh people. What the iBreastExam is doing is screening the asymptomatic population, funneling down the ones with positive findings that actually require a doctor's follow-up.
We are doing this through ASHA workers. If you ask why them: they are a great way to build relationships and create awareness. When you see a woman from your own community coming to your doorstep, saying, "I'm going to do a 7-minute test using the iBreastExam in your comfort zone," she becomes the awareness piece. At the end of the day, a woman is more likely to believe someone from her own community and trust them.
Can you share a specific incident or example of how this model works on the ground?**
The device is portable and completely battery-powered. You charge it like your regular cell phone, and on a single charge, it runs for about 12 hours. You can do at-home screenings, corporate screenings, or anywhere you can find a basic, small room with a bed to lie down. You don't need AC or any other infrastructural setup to administer the test.
We did a screening program in Gujarat recently, in collaboration with Gokuldham Nar, with a group of three trained operators who went to the villages, funded by the Helping Hands Virginia Foundation from the US. These women went door-to-door, screening women and creating awareness. If there was anyone whose test came up positive, she would be brought back to a district hospital for a follow-up checkup using a mammogram or ultrasound.
How easy or difficult has it been to collaborate and tie up with government bodies and hospitals?
HLL Lifecare is our implementation partner; they have been in the field for so long and wholly understand the need for early detection. When we talk about early detection, we are not just talking about saving lives but also saving money that would otherwise go into treatment from the government’s end.
We are currently working with the government of Goa. We have screened over 1.5 lakh women there, and we continue to screen because early detection of breast cancer is not a one-time thing; it's a year-on-year test. The government has made sure that any woman who tests positive on the iBreastExam will get all follow-up tests, including treatment, free of cost at the Government Medical College (GMC) in the State.
Similarly, we are working with all government medical colleges in Maharashtra. We have already completed one lakh screenings, and right now we are in phase two, where the colleges have repurchased scans and cartridges from us. Tie-ups with these GMCs allow us to close the loop end-to-end; not just detection, but treatment and follow-ups are included too. The government has been quite cooperative because we are using existing infrastructure, like PHCs (Primary Health Centres) and CHCs (Community Health Centres), and we are able to use ASHA workers, who are part of the government’s system. It's been good working with all of them.
As you expand, how do you manage the balance between quality and quantity during this growth phase?
You have ISO approvals and audits that happen routinely. It's teamwork. It's not just me; we have a phenomenal team, a majority of whom are women.
What role does Artificial Intelligence play in the functionality of the iBreastExam?**
AI does make a difference from the iBreastExam’s perspective. When we send an ASHA worker to screen a lady, our AI-enabled algorithm allows the operator to let the woman know if there is a finding or not right at the end of the screening. Had it not been AI-enabled, it would take time to process the reports. Then you'd have to find the woman with the positive instance all over again and convince her to come to the district hospital. Now, all of that happens all at once, so they move quickly.
How has the response been from the wider healthcare industry?
When it comes to any new medical technology, efficiency is important. The iBreastExam is at the same sensitivity and specificity, at par with mammography. As I mentioned from our study in India, in spite of hospitals having a mammography setup, you only see 1.3 per cent to 1.7 per cent of women coming for a checkup. Mammography right now is at a standstill, not helping us bridge the gap between those who get tested early and those who get tested at all.
If the iBreastExam were brought on board, you're helping create that primary screening segment. Whoever is positive will still come back to mammography for a follow-up, so you're also increasing footfall for early-stage detections. It's a good partner device for mammography. Plus, you can do outreach programs that are usually not possible with mammography, such as corporate, door-to-door, and at-home screenings.
Have you established any partnerships with private hospitals in India?
We have tied up with doctors, and we're working with certain private hospitals in Mumbai for their corporate screening arm. We also did a screening program through Hinduja Hospital for all the policewomen of Mumbai and their families. Since these women are too busy to come to the hospital, we dispatched the device to the police station. They were given a small room, and the women would come and go based on their availability.
When it comes to approaches, you can get as innovative as possible because we don't need infrastructure, not even a plug point, just a normal bed to lie on for about 5 minutes. You don't require gel, and it has no contraindications; even pregnant ladies can get it done. It's as safe as your cell phone because it uses similar technology: capacitive sensors, the same as your touchscreen phone, in a dynamic coplanar version. If a lady can use a cell phone, she can use the iBreastExam.
What are the future plans for UE LifeSciences?
For future plans, the idea is to grow partnerships because, as you mentioned, 2 million is not a big number from a reach perspective. The idea is to make this a standard of care so that every woman has access, can get herself screened, and bring down the number of breast cancer deaths in India.
As per GloboCan data, India was ranked highest in Asia for breast cancer deaths. If we could bring those numbers down, we're talking about protecting 50 per cent of our population, the productive segment of the community.
Got a story that Healthcare Executive should dig into? Shoot it over to arunima.rajan@hosmac.com—no PR fluff, just solid leads.