
Inverted Healthcare Pyramid: Why Specialists Are Triaging Skin Rashes
By Arunima Rajan

A critical lack of trust and quality in primary care is forcing millions to bypass local clinics, resulting in overburdened tertiary hospitals, duplicated costs, and a fragmented system.
Imagine you are a patient in a rural village in Madhya Pradesh. You have a chronic heart condition and have traveled six hours by bus and autorickshaw to reach a tertiary care hospital. When you arrive, the waiting room is overflowing with people suffering from minor issues like skin rashes, fevers, and coughs, conditions that could easily be managed by a primary care physician.
This happens primarily because there is no gatekeeper in India’s healthcare system. The result? The specialist who should be analyzing your ECG is instead triaging patients with minor ailments. Meanwhile, the patient who needs urgent care cannot even find a bed. This is the daily reality for hundreds of thousands of patients in India.
According to a Lancet study, 122 Indians per 100,000 die every year due to poor healthcare accessibility. The issue isn't just a lack of hospitals; it is that the wrong patients are landing at the wrong kinds of hospitals.
The Pyramid that Flipped
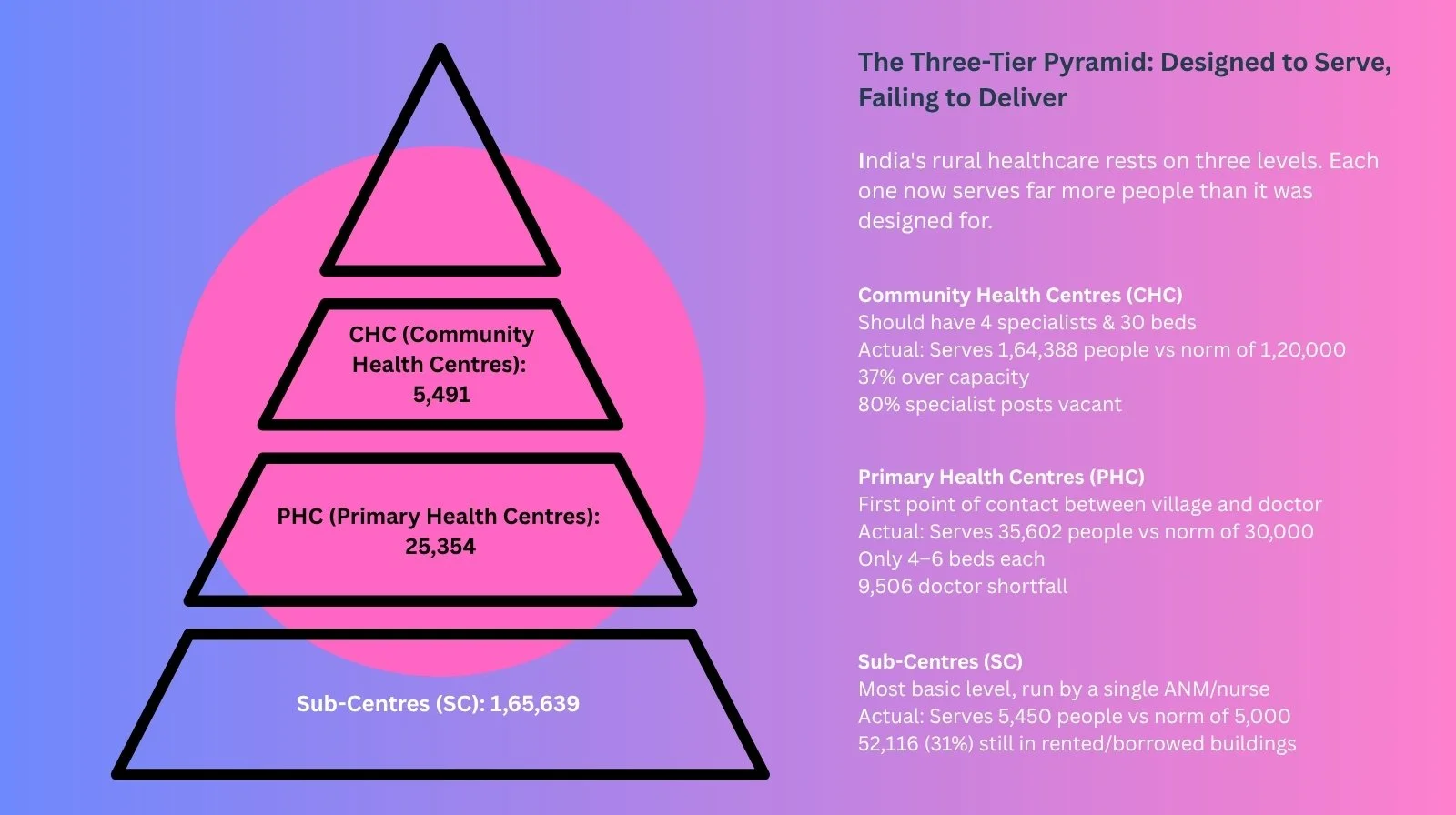
India traditionally utilized a three-tier healthcare "pyramid" focusing on primary, secondary, and tertiary care. The logic was simple: the broad base would absorb most cases, and only complex complications would be referred to the top.
Today, that pyramid is inverted. Patients bypass local clinics for tertiary centers like AIIMS or Tata Memorial because they offer "one-stop" access to diagnostics. Lower tiers have failed to earn trust due to persistent governance gaps.
Dr. Praveen Muralidharan, a senior nephrologist and medical superintendent at KIMSHEALTH Thiruvananthapuram, sees the consequences daily. “Understaffing, overcrowding, and eroding trust push patients toward tertiary centers,” he says. “Primary care physicians themselves often refer upward for minor conditions, driven partly by litigation fears.”
Fragmented Delivery and Uneven Quality
“India’s three-tier healthcare pyramid isn’t failing because the model is flawed; it’s failing because the first two layers haven’t earned patient trust,” says Mayank Banerjee, Co-founder of Even Healthcare.
In reality, the system lacks integration. A primary care doctor rarely coordinates with secondary care, and by the time a patient reaches a specialist, there is no continuity of context. This leads to the duplication of tests and costs.
“When primary and secondary care lack consistent quality, patients naturally bypass them for speed and certainty,” Banerjee adds. “The consequence is that tertiary centers become overburdened, and patients end up overpaying for specialized care they may not even need.”
The Trust Deficit
Malini Bharathi, a former HR professional, explains the shift in simple terms: “Earlier, families stayed in the same locality for generations. There was a neighborhood clinic where everyone knew the community doctor.”
That world has vanished. Living in a new suburb of Chennai, Bharathi doesn't know the local doctors. “I prefer Apollo Hospital because everything is under one roof. They have all my data: from surgeries to reports, so it’s easier to consult a doctor who knows my background.”
Multiply Bharathi’s experience by millions, and the congestion at the top becomes inevitable. It isn't irrational behavior; it is a logical response to a fragmented system.
The Market Fills the Vacuum
While the public sector struggles to sort patients, private capital is building shortcuts. Single-specialty hospital chains grew from 20% of India’s hospital market in 2019 to 30% by 2024, according to Moneycontrol.
An Avendus Capital 2025 analysis projects this will reach 40% by 2028. This growth is the market realizing the opportunity created by the "broken pyramid." When a patient cannot trust a district hospital to treat a kidney issue, a nephrology chain with same-day diagnostics becomes the obvious choice. The patient becomes her own referral system.
The Money Problem
Is this a resource problem or a management problem? Ravi Duggal, a public health researcher, argues it is both.
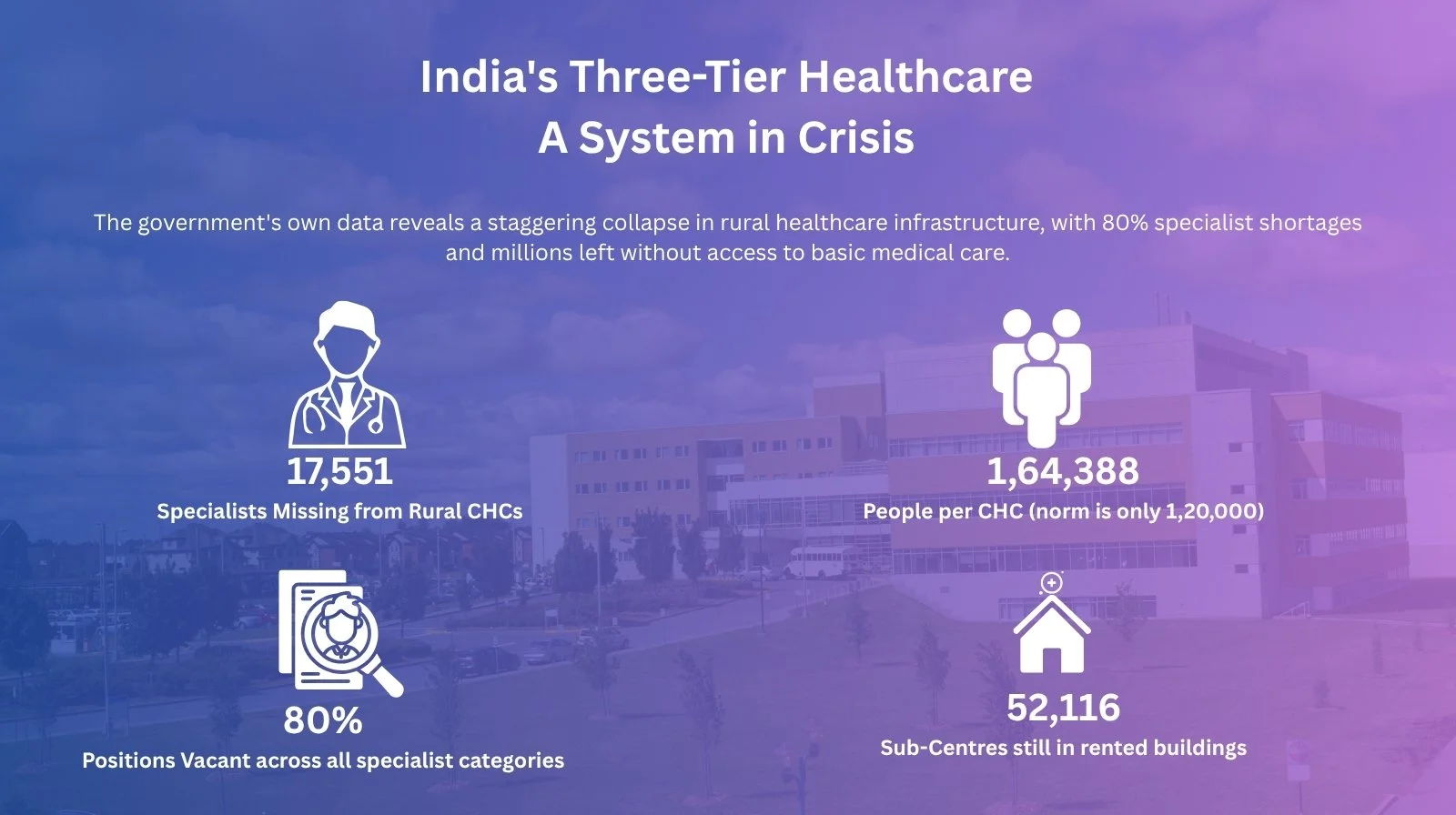
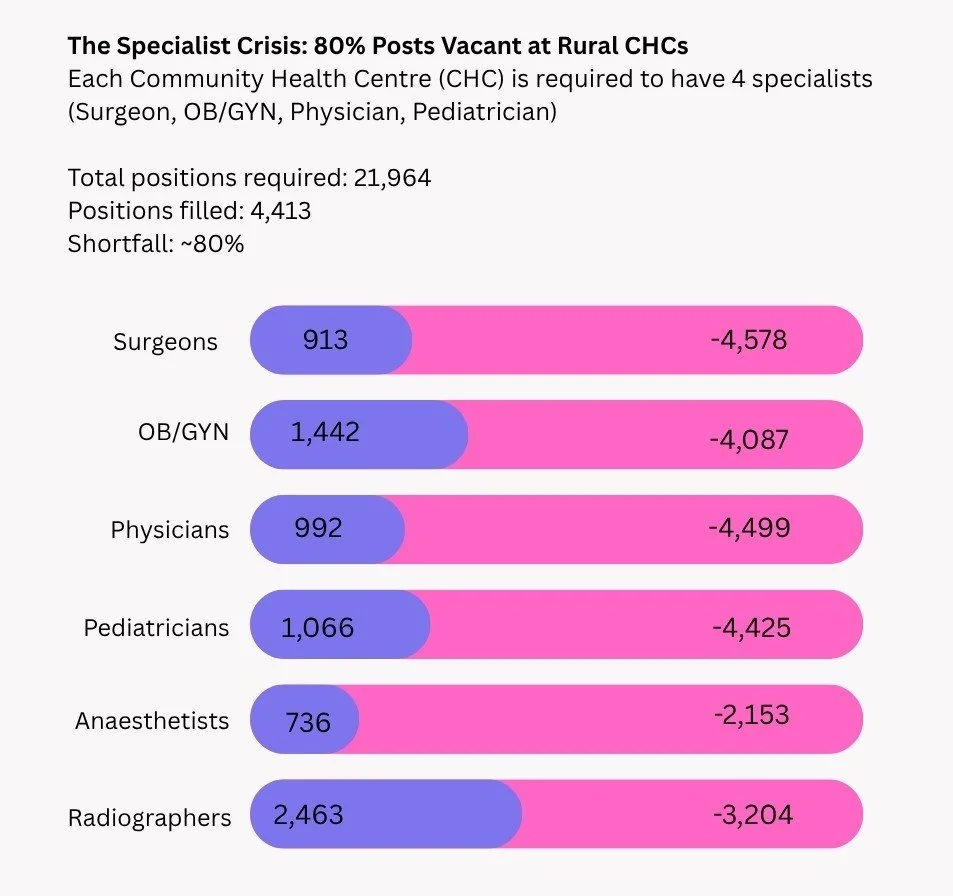
“India has not invested enough in a robust public system. Budgets are ridiculously low, only 1.2% of GDP, despite the National Health Policy mandate of 2.5%,” says Duggal. Consequently, facilities are chronically understaffed. “In primary healthcare, doctor shortfalls reach 40%. At the rural hospital tier, over 70% of specialist positions are vacant.”
The PMJAY Paradox
The Pradhan Mantri Jan Arogya Yojana (PMJAY) was designed to protect citizens from "catastrophic" health expenses. However, Duggal points out a paradox: it has largely become a funding mechanism for private healthcare.
“About 70% of PMJAY patients are treated in the private sector,” he explains. “Instead of investing in public facilities to build credibility, the government is redirecting limited resources to private beds.”
The CGHS Question: A Tale of Two Citizens
Duggal notes a stark disparity in how the government values its citizens. The Central Government Health Scheme (CGHS), which covers bureaucrats, MPs, and judges, spends roughly ₹18,500 per capita. For the rest of the population, the Ministry of Health spends only about ₹2,500 per capita.
“Why this discrimination?” he asks. He points to neighbors like Thailand and Sri Lanka as models for universal access. Some Indian states, such as Mizoram, Goa, and Himachal Pradesh, are already investing over ₹5,000 per capita and seeing better results because their public systems are forced to respond to the lack of a private sector.
Duggal’s prescription is blunt: double the healthcare budget, remove user fees, and mandate a "Right to Healthcare" through legislative action.
Access is Not the Same as Care
India’s healthcare diagnosis is clear: a collection of facilities with uneven quality and no accountability for outcomes. The fix must happen at the base.
Dr. Muralidharan points to an uncomfortable truth in Kerala. Despite a high Universal Health Care rating, the state has a high prevalence of diabetes and hypertension. “This demonstrates that access alone does not guarantee the ability to manage chronic disease,” he says.
The Verdict: India needs a different kind of primary care, one focused on chronic disease management, data continuity, and a robust referral system that actually works.
Got a story that Healthcare Executive should dig into? Shoot it over to arunima.rajan@hosmac.com—no PR fluff, just solid leads.