
India Trains Nurses for the World, but Fails Its Own Patients
By Arunima Rajan

To Address the Nursing Shortage, India Needs a Complete Healthcare Overhaul
Indian nurses are respected across the world. The remittances they send home support families and strengthen the national economy. Yet, by failing to improve their working conditions, we are silently accepting a system where Indian patients receive compromised care while other countries benefit from our trained workforce.
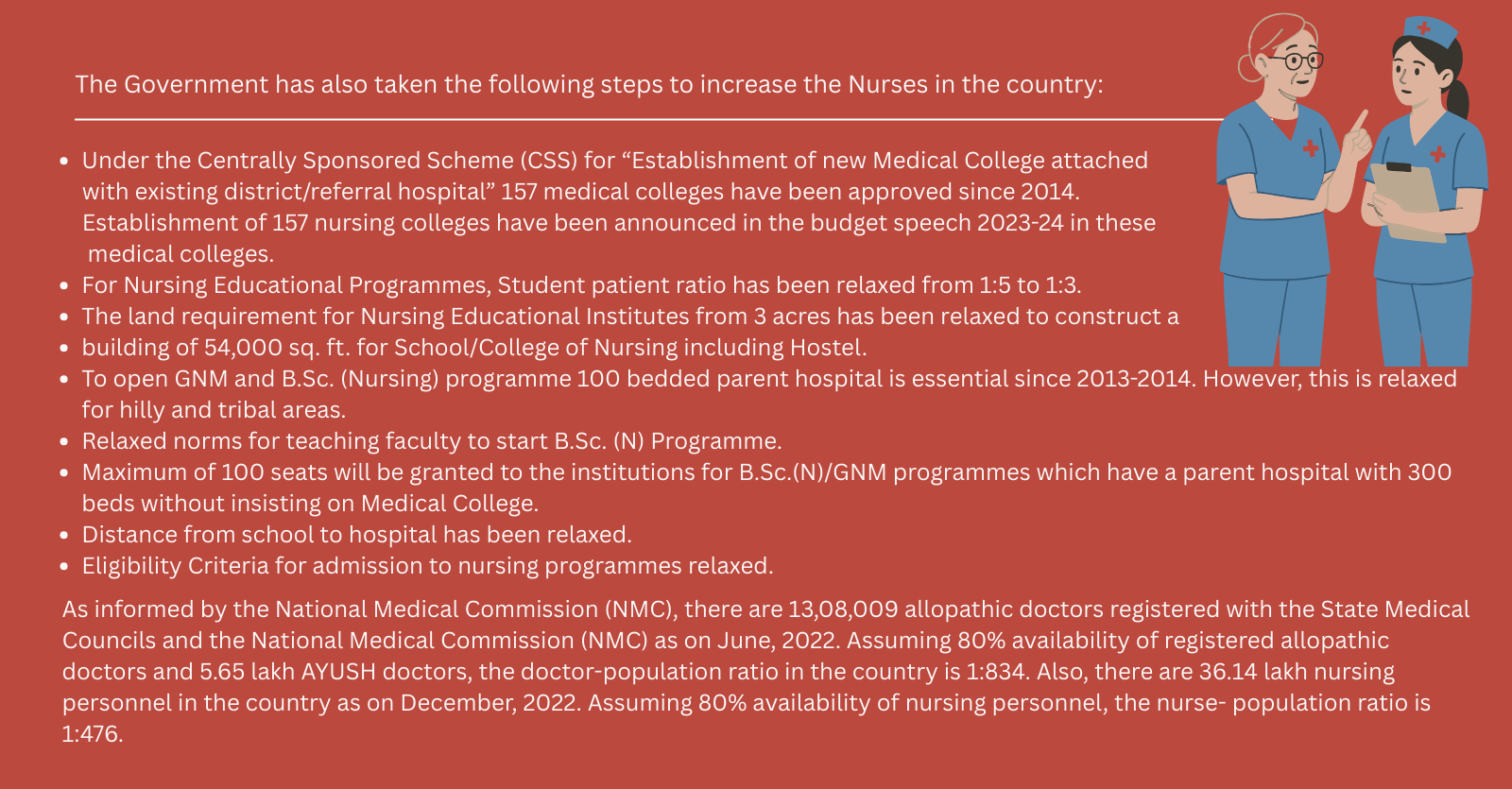
The WHO benchmark for nurse density is 3 nurses per 1,000 population. India, however, has only 1.7–2 nurses per 1,000, leaving an estimated shortfall of nearly 2 million nurses. This gap is felt most acutely in small towns and rural areas, where nurses increasingly migrate to the Middle East, the UK, and other countries in search of better opportunities.
High Attrition and Migration
“I had a very efficient nurse who trained with me, but she moved to Dubai and is now the Head of Nursing in the Gynaecology Department at Aster Hospital,” says Dr Omana Rajan, Managing Director of Life Care Family Health Clinic and Diagnostic Centre, Kottayam, Kerala.
“The attrition rate is extremely high in smaller towns. We hire every six months because we simply cannot retain staff.”
The situation is even more severe in government hospitals, where working conditions, pay, and infrastructure challenges further accelerate migration and attrition.
Lack of Clinical Exposure and Training Gaps
According to Saly Suseel, Director of Nursing at Dr L H Hiranandani Hospital, Mumbai, the healthcare system itself pushes nurses away.
“Nursing colleges have grown rapidly, which has helped increase numbers, but many students graduate with little hands-on clinical experience. When they join hospitals, they are immediately placed in overcrowded wards, with too many patients, long hours, low pay, and little respect. Many burn out quickly. Some leave the country, and some leave the profession entirely.”
The Clinical Cost of Nurse Shortages
When nurses are overstretched, patient care inevitably suffers. Basic but critical tasks—timely monitoring of vital signs, accurate medication administration, infection control—are rushed or missed. Hospital-acquired infections rise, recovery slows, and patients remain hospitalised longer than necessary.
“It becomes a vicious cycle,” explains Beena K T, Nursing Superintendent, Kinder Women’s Hospital and Fertility Centre, Bengaluru.
“Short staffing leads to longer shifts, burnout, and illness among nurses. Infection rates rise, performance declines, hospital reputation suffers, and attrition increases further. The system collapses inward on itself.”
She adds that nurses must be treated as trained clinical decision-makers, not merely support staff.
“Research shows that when nurses are empowered with autonomy, leadership roles, and authority in care planning, patient outcomes improve and burnout reduces.”
Why Temporary Fixes Don’t Work
Hospitals often turn to agency or temporary nurses to manage staffing crises. While this may offer short-term relief, it creates new problems.
Agency nurses lack familiarity with hospital protocols, require repeated orientation, and disrupt continuity of care. Accountability weakens, patient safety risks increase, and permanent staff morale suffers. Financial costs rise without solving the structural problem.
In short: shortcuts worsen the crisis instead of fixing it.
A Broken System Cannot Retain Its Workforce
Mathew George, Professor of Public Health and Community Medicine, Central University of Kerala, explains that nurse shortages cannot be viewed in isolation.
“Nurse shortages only become visible when systems have adequate doctors, beds, and infrastructure. In many public facilities, infrastructure inadequacy hides workforce shortages. We also fail to clearly define the different categories of nurses and their roles.”
He highlights the lack of structured professional pathways, such as nurse practitioners and midwifery-led care models, which are well established in countries like the UK. While some Indian institutions, such as the Fernandez Hospital in Hyderabad are working toward this model, systemic adoption remains limited.
Structural Reform, Not Cosmetic ChangeWorkforce
Rashmi Rajiv Sawant, Chief Nursing Officer, Gleneagles Hospital, Mumbai, notes that the shortage is not caused by a single factor but by interconnected failures:
Low remuneration
Long and irregular working hours
High patient-to-nurse ratios
Poor career progression
Limited leadership roles
Lack of professional autonomy
Inadequate recognition and respect
“Nurses and doctors are complementary pillars of healthcare, but nurses experience a persistent imbalance in recognition, autonomy, and decision-making authority. Over time, this leads to emotional exhaustion and burnout. Many migrate abroad, and many discourage future generations from entering the profession.”
Sawant emphasises that restricting migration is not the solution.
“We cannot stop young professionals from going abroad. Retention will only improve when we create working conditions where nurses feel valued, respected, professionally fulfilled, and fairly compensated. We need competitive pay, structured career ladders, leadership roles, and globally aligned education standards that still serve local healthcare needs.”
Nursing Is an Investment, Not an Expense
As Saly Suseel puts it: “Fair pay, safe staffing ratios, decent accommodation, respect, and career progression are not luxuries. They are basic requirements for quality patient care.”
Unless India reforms its healthcare system structurally, it will continue to train nurses for other countries while Indian hospitals remain understaffed.
The Way Forward
Real solutions require systemic change:
National minimum nurse–patient ratio norms
Permanent posts in government hospitals
Structured clinical and leadership career ladders
Recognition of advanced nursing roles (nurse practitioners, midwifery models)
Ethical bilateral recruitment agreements with return pathways
Standardised, high-quality clinical training
Respect, autonomy, and decision-making authority for nurses
India may not reverse nurse migration—but it can stop bleeding its workforce.
Without deep reform, every quick fix will fail.
The nursing crisis is not a staffing problem—it is a system failure.
Got a story that Healthcare Executive should dig into? Shoot it over to arunima.rajan@hosmac.com—no PR fluff, just solid leads.