
Built to Fail: How Our Infrastructure Is Fueling India's Heat Crisis
By Arunima Rajan

A leading urban health expert explains why our cooling strategies are backfiring, and why the fix is a matter of political will, not just technology
Ronita Bardhan, professor of sustainable built environment and health at the University of Cambridge, United Kingdom.
Where are you from, and why do you do what you do?
I was born in Calcutta, lived a brief stint in Delhi, and grew up again in Calcutta, I should say Kolkata. These cities taught me how heat, humidity, and crowded infrastructure can affect people's lives. Currently, I am a Professor of Sustainable Built Environment and Health at the University of Cambridge, where I lead the Sustainable Design Group. Trained as an architect and urban engineer, I spent years working on Indian cities before establishing my research group. We work at the intersection of buildings, the built environment, climate, and health, based on a simple conviction: the places we design either protect or harm people. If we choose better designs now, I believe we can protect a large population who probably did not contribute to climate change in the first place. Intervening in the built environment is the only agency we have as humans because we plan our cities. If we build them to be sensitive to people’s health and lived experiences, we give every citizen an equal opportunity to live well.
Why is it so hot this year, and what is really driving this spike in heat?
The primary reason is the accumulation of greenhouse gases caused by fossil fuel burning. However, the extreme events we are seeing now will be the "new normal." They will amplify and occur more frequently. Beyond trapping heat, our urban living habits prevent the radiation from cooling off. It becomes trapped in our built infrastructure: cities, roads, and buildings. The more we build and remove natural heat sinks, the more we create heat sources. All air conditioning units are heat sources; they cool our indoors while venting heat to the outdoors, which we call "anthropogenic heat." This accumulation creates higher temperatures during the evenings and nights, preventing our bodies from recovering. At the city level, this creates "heat-island effects." In Mumbai, we detect a temperature difference of 3 to 8 degrees compared to rural counterparts. While fossil fuels are the foundation, urban planning, land use, and natural climate variability are significantly amplifying the crisis. This is something we can control.
What would be an example of a heat sink?
A park, a water body, or a national reserve forest. Even vertical greening can act as a heat sink. Anything that withdraws heat from the atmosphere or prevents it from reflecting back functions as a heat sink.
How can hospitals reduce their energy consumption?
It is a genuine paradox. We are treating people who have fallen sick due to extreme heat, but to do so, we rely on heavily air-conditioned spaces. In the UK, the National Health Service (NHS) accounts for roughly 4-5% of national carbon emissions. The solutions exist and are increasingly cost-effective. Passive design, orienting buildings to avoid direct solar radiation, can cut cooling loads by 30-40% without active technology. Solar rooftops combined with battery storage are economical and scalable. In India, with over 3,200 hours of sunlight annually, harnessing this energy is a no-brainer. Not doing so is an institutional failure, not a resource failure.
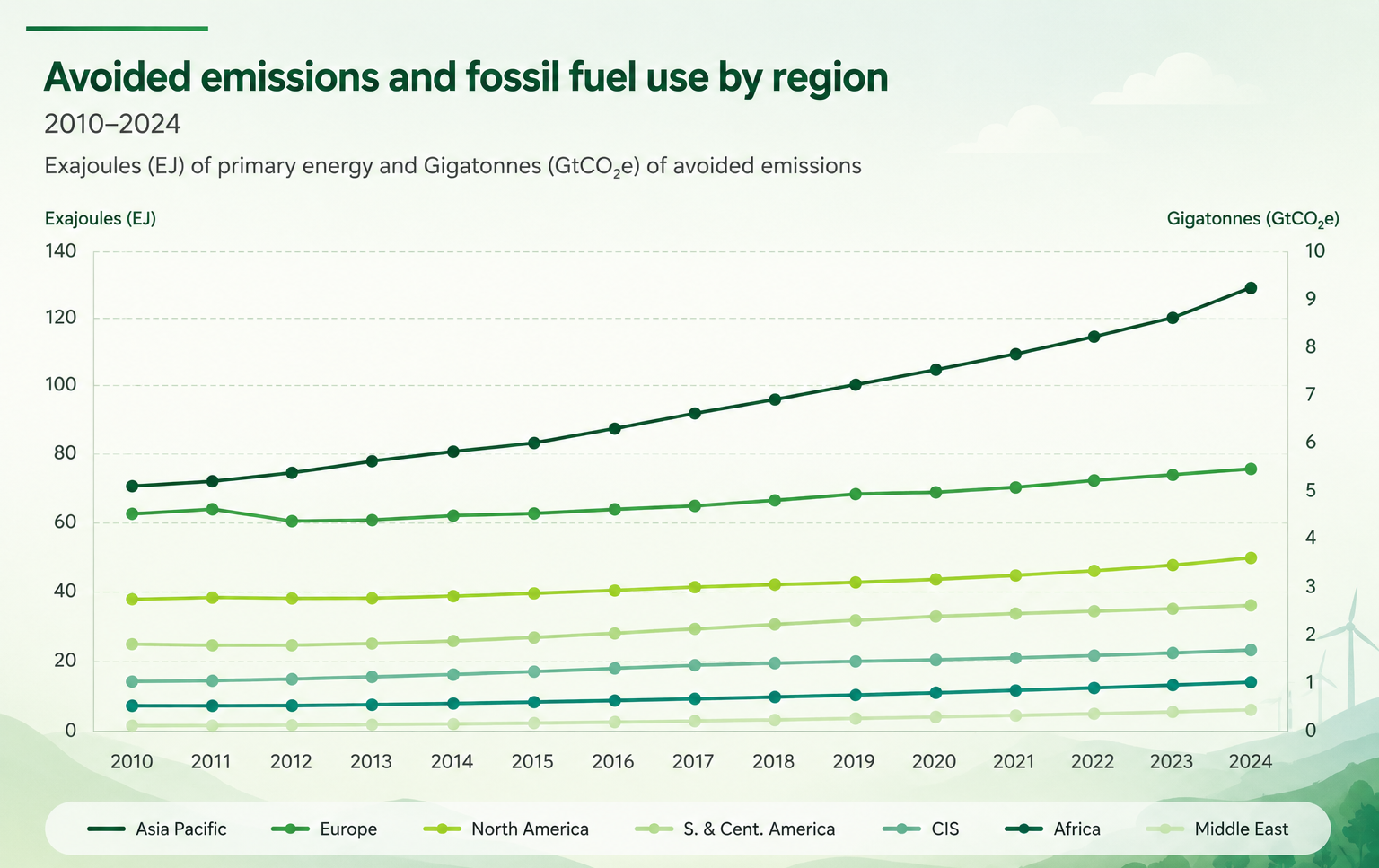
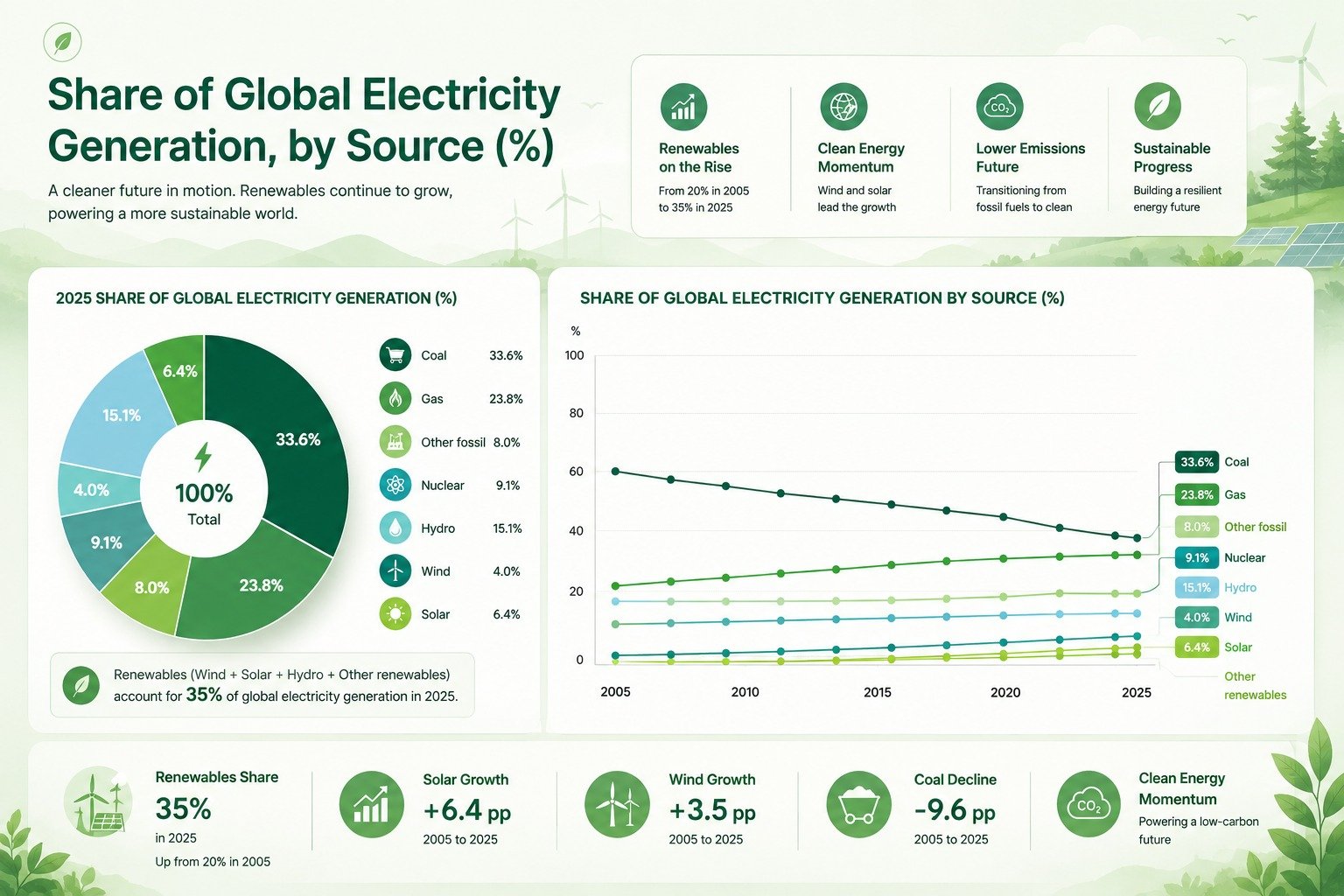
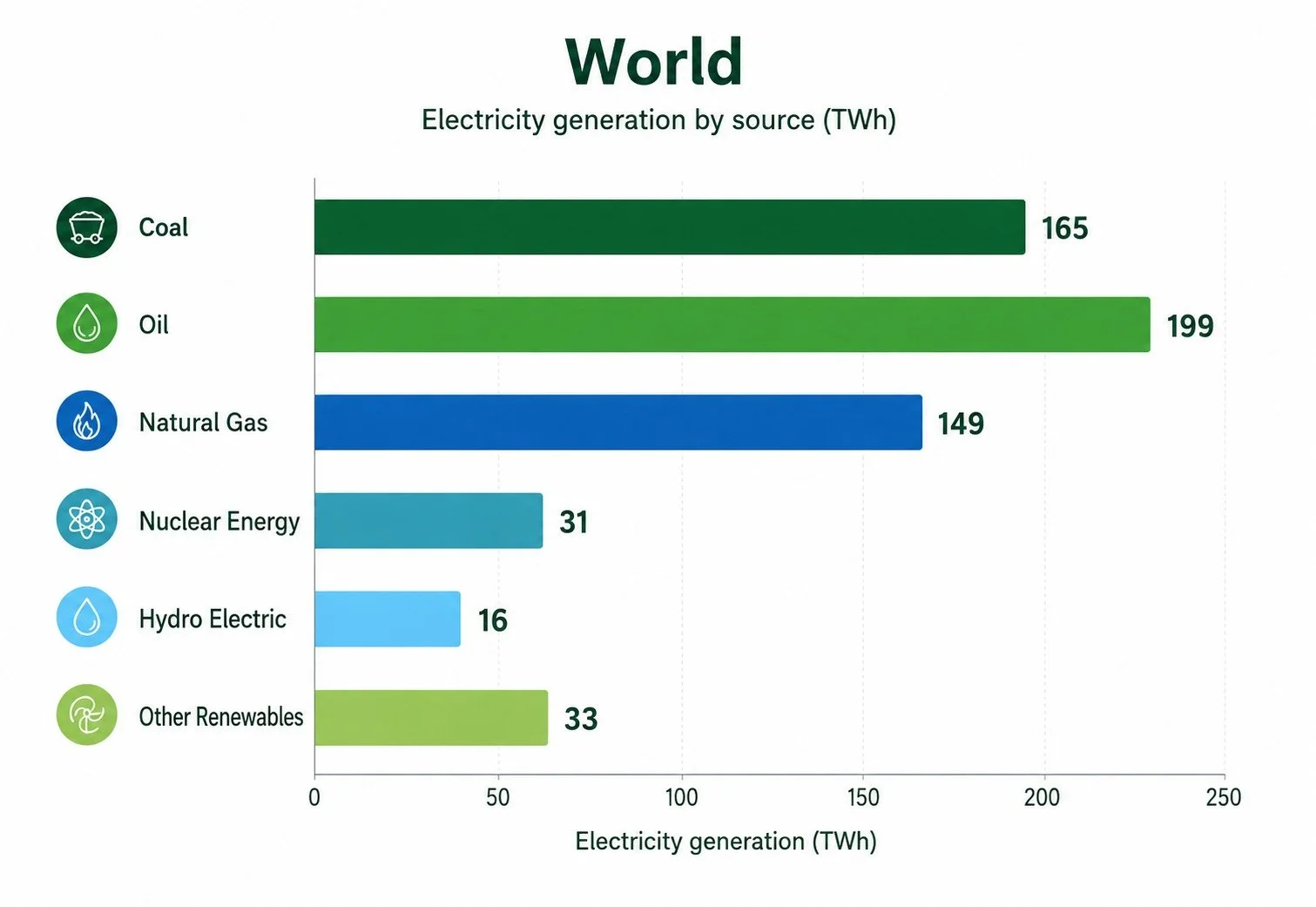
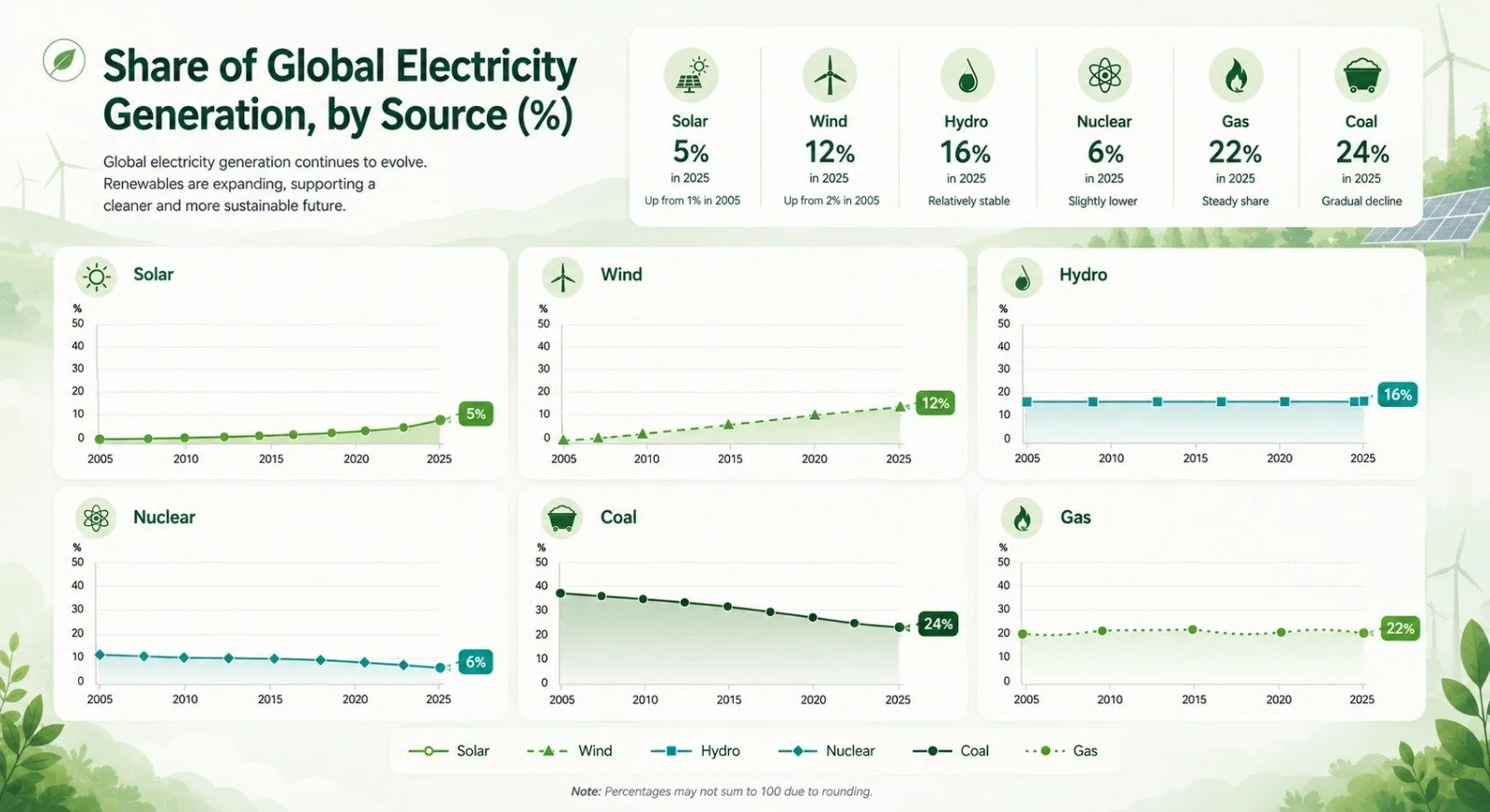
Source: Energy Institute Statistical Review of World Energy 2025
People wait for hours outside to see a doctor. How can you incorporate better design into public hospitals?
Last year, I worked on a project tracking public hospitals in Bihar. We installed temperature sensors in triage areas and recorded abnormally high levels. Hospital queuing during a heatwave is a predictable yet preventable harm. The fact that this is recognized in cities yet remains unaddressed is an institutional failure. Immediate interventions could include low-cost shaded areas to keep people out of direct sun. Our research shows that pregnant mothers living in higher ambient temperatures have different birth outcomes than those in cooler environments. There is also an urgent need for staff training, as those working in these environments are doubly jeopardized by the heat while handling high patient volumes. Identifying vulnerabilities and prioritizing the most at-risk individuals is essential.
Are our buildings designed for women? What are the most glaring gaps?
The fundamental gap is that our building codes and design standards are based on 1950s English standards. Thermal comfort metrics are calibrated on metabolic rates that systematically underestimate the heat sensitivity of women. In my work, I treat design as a preventive strategy, a form of "precision medicine", rather than just a physical structure.
What would it take for clean energy alternatives to become the default?
First, we must identify that healthcare falls under different ministries across various states. Second, there are currently no incentives for facility managers to implement alternative cooling methods or prioritize energy savings. Third, we need comprehensive training, awareness, and education programs, especially in Tier 2 and Tier 3 cities.
What is the Rahat Initiative?
It is a project I spearhead as the principal investigator, funded by UK Research and Innovation. Much like a medical trial, we used built environment interventions as the "medicine." We selected 80 homes and painted the roofs of 40 of them white. We worked in Jodhpur, which experiences some of the highest temperatures, partnering with NGOs that provide housing credit to low-income women.
Do they also use blue paint on the walls to reduce temperature?
That was a traditional method, which is why we have "Blue Cities." Today, with better technology, we have paints that reflect significantly more light and heat. We created a policy "menu card" for policymakers to see which interventions work best for specific building types, and we developed a comic book to build public awareness.
What was the finding regarding the impact of heat on women?
Women and men’s heat coping mechanisms are different. Because thermal comfort standards were developed based on the "average" 6-foot-tall male, a standard popularized by Carrier in the 1960s, they do not account for these physiological differences. Menopausal or perimenopausal women also experience extreme body heat. We found that while their indoor temperatures were elevated, their skin temperatures were constantly high. We are now working to monitor core body temperatures.
Do Indian cities have an action plan?
Many have them, but 137 cities across India have Heat Action Plans that are not comparable to one another.
What exactly is a heat action plan?
It is a dual-purpose strategy that responds to both chronic heat and acute heatwaves. I am currently advising the Mumbai Metropolitan Region Development Authority (MMRDA) on the development of the Maharashtra Heat Action Plan.
Do these fields work in silos, or is it possible for them to work together?
When productive people die due to climate events, it is a loss for the city. Governments now recognize that this is a multi-sectoral problem affecting everything from economics to health and education. Even schools are noticing a difference in how children learn during heatwaves. It is no longer a siloed discussion, at least not in major city governments.
Many people continue their routines during extreme heat. How can we improve adherence to advisories?
This is a matter of education. In Kolkata, when pollution levels were high, the government used a traffic-signal-style lighting system to communicate risk, which was highly effective. Accessible information helps. Rajasthan has used jingles to communicate, even adding specific warnings during extreme heatwaves.
How do you treat heat like an emergency?
First, the government must formally classify heat as a disaster category, similar to how the National Disaster Management Authority (NDMA) treats floods and cyclones. Second, we need a national heat mortality register or a surveillance system; currently, there is no standardized medical protocol to identify a death as heat-related. Third, we must designate responsive healthcare settings for large gatherings and build infrastructure like hydration points and 24-hour heat helplines. Embedding cooling infrastructure is a matter of choice, not a constraint. Designing a better city is not a luxury—it yields immense co-benefits.
What lessons can India learn from the UK's approach?
The UK’s preparedness is high, and there is clear policy-level cognisance. They generate evidence and provide structured research funding. I am also working in Singapore, where there is clear political will focused on reducing the number of elderly patients ending up in hospitals. That is the kind of commitment we need.
Got a story that Healthcare Executive should dig into? Shoot it over to arunima.rajan@hosmac.com—no PR fluff, just solid leads.