
Assessing IAQ in an ICU: A Case Study
By Krutikaa Sharma

The study neatly identifies the factors that influence IAQ in an ICU of a metropolitan hospital.
Building owners, designers and operators are challenged to reduce the environmental impacts of buildings, including energy consumption and associated greenhouse gas emissions, while maintaining indoor environments that are conducive to occupant health, safety and productivity. As the patient’s health is the most critical factor in an ICU, the need for maintaining a good indoor quality is of paramount importance. The ventilation system provided and outdoor ambient conditions directly impact the indoor air quality in the space. Usually, in practice, with the aim of achieving better air quality, the ventilation systems are overdesigned to generate air changes that is greater than what is actually required or recommended by the standards. In doing so, there is a tremendous consumption of energy, which is footed by the healthcare organization but a part of it by the patients too.
According to a study by Capolongo et al. In 2016, fine particulate matter (PM) pollutants from numerous sources have been implicated in acute respiratory diseases. There is a popular belief that contamination control demands high ventilation rates. This study evaluates the time-based variations in the particulate matter concentrations in the indoor air in a medical ICU of a metropolitan hospital. It mainly investigates the impact of the VRs through indoor air quality procedure (IAQP) in the units, on the patient exposure to the concentration levels of the particulate matter.
Simultaneously considering energy, airflow rates and Indoor Air Quality (IAQ), reduction of the total air change requirements (at potential hours identified through the study) could provide a great opportunity to significantly reduce energy consumption and maintaining good indoor air quality. According to a study by Emmerich and Persily in 2001, while energy is critically important, it is only one aspect of building performance and should not be pursed to the neglect of IAQ that affect building occupants. Source control also offers the potential to reduce outdoor air Ventilation Rates (VR), which can save energy for space conditioning. Such reductions are allowed under the IAQP of ASHRAE Standard 62.1 – 2013 (ASHRAE, 2013). This was done by the performance-based approach IAQP approach defined in ASHRAE standard. This study would greatly benefit healthcare organizations in reducing their energy footprint but more importantly the health of the patient.
Indoor Air factors in Intensive Care Units
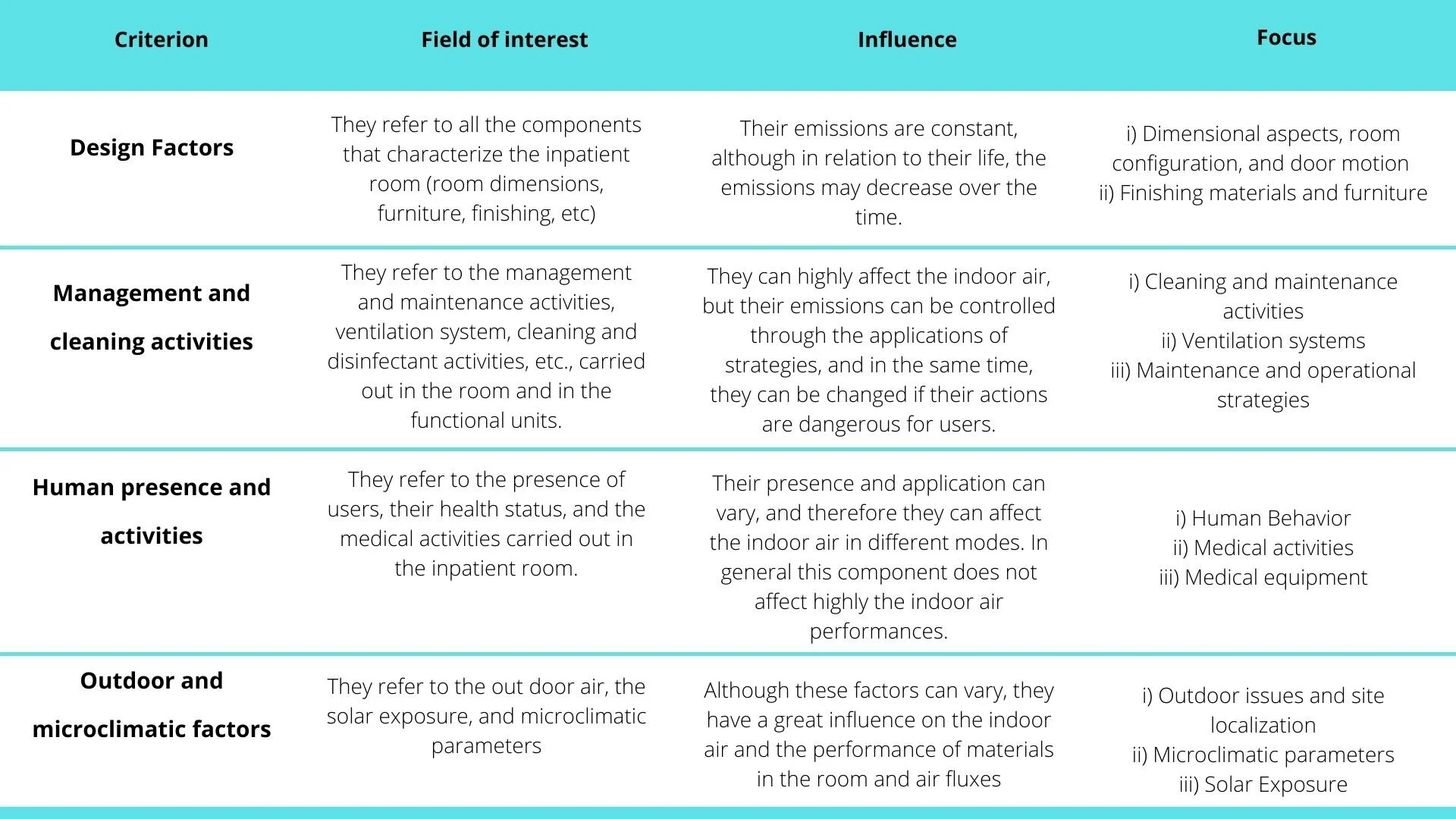
Table 1: Factors influencing the Indoor air in the Intensive Care Units
The above parameters of healthcare facilities are defined by specific standards, which have evolved over the last decades. ASHRAE 170 defines the following values;
Temperature in the intensive care units should be between 21 – 24 ͦC
Relative humidity in intensive care units, if possible in the air-locks, should have a range between 40-60%
Air changes – it must be able to achieve and maintain the air quality and movement conditions. The values should be, for outdoor, 2 ACH (Air change rate minimum) and, totally, 6 ACH.
Ventilation System – the outdoor air flow rates for hospitals, intensive care units are mostly 30 % outdoor air intake, unless specified for isolation rooms and operation theatres.
Air velocity – should vary between 0.05 m/s and 0.25 m/s or no more than 0.30 m/s can be detected.
Air filtration – classification in fourteen filter classes, for different types of wards and services, these range from a minimum of 6 to a maximum of 12, however, with a filtration efficiency of at least M + A (medium-high)
Pressure – The minimum pressure difference between rooms and corridors and rooms and toilets is usually about 2.5 Pa.
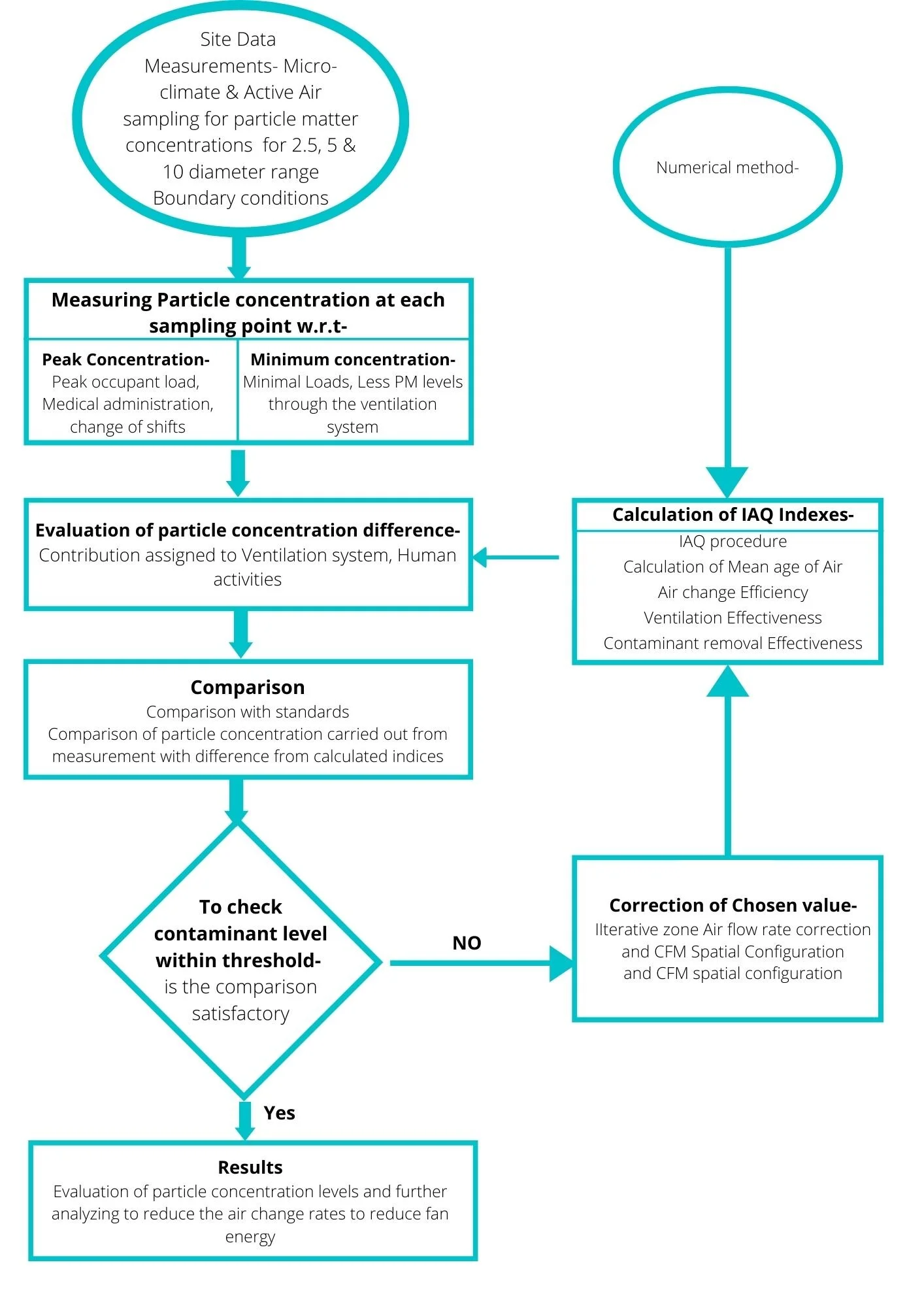
Study Methodology
Referring to a few specific case studies and suggestions for good practices, a methodology was drafted to undertake the study.
Healthcare Ventilation Standards & Contaminant thresholds
Ventilation requirements are on the basis of the standards of air quality for hospitals. The standards give the values for the temperature, relative humidity, air change rates, types of filters, the pressure relationship to adjacent areas and the cases where recirculation of air is allowed. All these requirements are classified according to the purpose of the premises to meet the requirements of patients, staff and to resist the contaminant.

Table 2: ASHRAE 170 Standard for Ventilation in Healthcare requirements

Table 3: Comparison of different standards for Particulate matter and Carbon dioxide levels
Air Filter Efficiency
A number of studies, by Passweg et al & Sherertz et al in 1998, showed that high air cleanliness can reduce the rate of infection for high-acuity patient groups; for example, HEPA-filtered isolation rooms. According to Friberg et al in 2003 & Hahn et al in 2002, Air contaminants are minimal with the use of HEPA filters with laminar airflow, which are recommended for critical areas such as isolation rooms, operating rooms and intensive care units. Proper selection of air filtration is important to obtain good performance and cost management for ventilation system.
The Study
Many prior studies, for example by Pope et al in 1995, have established that many air pollutants are present in the air but most important is particulate matter which is responsible for cardio-vascular ailments. Particulate pollution in healthcare facilities is a potential threat to healthcare workers, patients and visitors. In this thesis, a study was carried out to monitor particulate levels in significant locations in the ICU of a secondary healthcare facility, in the Metropolitan area of Mumbai city. This hospital was chosen specifically to study the impact of the surrounding settings (heavy traffic, dense built-up area, parking) as well as the daily internal activities on the IAQ in the critical space through the ventilation system. Data were collected during the month of February 2020 for 3 continuous weeks through ATMOS equipment.
ASHRAE Standard for prescriptive “ventilation rate procedure” and its performance-based approach of IAQP help determine minimum VR based on objectively evaluated IAQ. This procedure helps to calculate both zone-level and system-level outdoor airflow rates.
The primary goal of this study was to determine, in the ICU, the adequacy of VRs (through the existing HVAC system) observed through measurements in providing the level of IAQ specified through the IAQP process. The second goal was to evaluate whether VRs implemented experimentally would achieve adequate IAQ, assessed objectively & subjectively (although subjectively is for the future scope of this study).
For the first goal, the contaminants of concern (selection was made considering the most critical one to health and respiratory concern – PM2.5 and microbial profile for infection risk) and reference exposure levels (RELs) was selected for evaluating IAQ. VR and indoor and outdoor contaminant concentrations were measured in the ICU. Mass balance models were employed to calculate indoor contaminant generation rate within the ICU. Using this model, the typical outdoor air contaminant concentrations, mass balance model was again used to calculate the ventilation rates that would maintain indoor contaminant concentrations below the selected REL. These VRs were compared to the measured VRs and the prescribed VRs in ASHRAE 170. An experiment is performed to check if by applying the IAQP to allow lower VRs in the considered zone, energy savings are possible whilst still maintaining acceptable IAQ.

Site Measurements
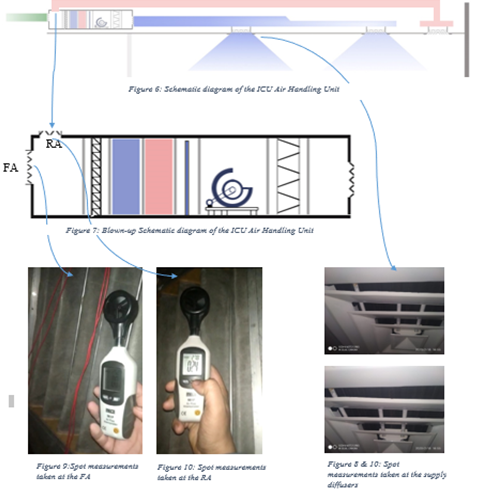
Spot Measurements
Based on the findings from applying the IAQP calculations and through an experimental performance optimization in the ICU, recommendations are made with regards to energy saving potential.
Measurements (at the patient breathing zone) indicated that hourly mean concentrations of PM2.5 in the ICU were 85-90 µg/m³ ± 3.5 during shift changes, 65 µg/m³ ±5.6 during relative visits, 60 µg/m³ ±2.6 during Doctor’s visits and 55 µg/m³ ±3.8 during Lunch & Medical administration. Concurrently particulate matter was monitored at the outdoor air intake and high levels of PM10 & PM2.5 were measured due to peak hour traffic and parking. Due to these elevated levels of PM outside & inside at the ICU at the patient breathing zone, a strategy was implemented where the airflow rates in critical zones were corrected and validated with respect to the particle matter concentration.

Graph showing particle matter concentration after modification of the CFM from 300 to 45o

Results & Observations- VRs were kept the same as per the standards, although increasing the zone air distribution effectiveness help control the particulate matter below REL, at the patient breathing zone. As the Outdoor particle concentrations vary significantly from day to day (and also predicted by season), along with major indoor activities, the air particle matter contaminants did rise a bit above the threshold value limit of 35 µg/m³ during major activities and peak traffic hour, nevertheless, results showed the suitability of the ventilation system in providing the expected air quality, if not all the time, most of the time.
Conclusion
Having a knowledge of the interactions and significance among IAQ parameters as determinants of building indoor environmental performance will enable the incorporation of more effective and reliable design strategies by system designers. IAQ contribution to building performance is such that it also contributes to a building energy performance. In designing HVAC building systems with the focus of achieving better IAQ, the issue of energy efficiency will be addressed.
One main contribution of this research to the body of knowledge existing is the development of a methodology to identify the parameters in an existing HVAC system to access the IAQ and thereby improving patient contaminant exposure while also considering energy. The aim for this study is for the devised methodology to provide a better, robust and clear-cut solution to the parameters weighing their contribution to measure IAQ performance in hospital buildings.
Hence, this study focusses on increasing the IAQ, a part of indoor environmental quality such that it also contributes to the building energy performance. This study strives to acknowledge that in designing HVAC building systems with the focus of achieving better IAQ, the issue of energy efficiency will be addressed.
Authors:
Krutikaa Sharma

Krutikaa Sharma is an architect from Mumbai, on her journey towards energy conservation through built forms. Upon completion of her bachelor of Architecture from Mumbai University and her masters in Building Energy Performance from CEPT University, she was a part of many urban healthcare projects. From then on, started a curiosity of integrating health infrastructure with disease resiliency and energy efficient systems to make healthcare in India a sustainable sector.